Objective: Recently, several epidemiologic studies reported that lithium in drinking water may be associated with lower rates of suicide mortality at the population level, but other studies failed to confirm the association. The objective of the present study is to determine whether lithium in drinking water is associated with lower suicide rate after adjustment of potential confounding factors.
Method: From 2010 to 2013, 274 mean lithium levels of 434 lithium samples in drinking water were examined in relation to suicide standardized mortality ratios (SMRs) in 274 municipalities of Kyushu Island in Japan. Weighted least squares regression analysis adjusted for the size of each population was used to investigate the association of lithium levels with suicide SMRs. The associations of lithium levels in drinking water with suicide SMRs (total, male, and female) were investigated adjusting for proportion of elderly people, proportion of 1-person households, proportion of people with college education or more, and proportion of people engaging in primary industry (adjusted model 1), and further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature, and annual postal savings per person (adjusted model 2).
Results: Lithium levels in drinking water were significantly (β = −.169, P = .019) and inversely associated with male suicide SMRs but not total or female SMRs in the adjusted model 2.
Conclusions: The present findings suggest that lithium in drinking water may be associated with the low risk of male suicide in the general population. Further studies are required to confirm these findings and investigate gender differences.
See Commentaries by Sher and Kapusta and König

Low Risk of Male Suicide and Lithium in Drinking Water

ABSTRACT
Objective: Recently, several epidemiologic studies reported that lithium in drinking water may be associated with lower rates of suicide mortality at the population level, but other studies failed to confirm the association. The objective of the present study is to determine whether lithium in drinking water is associated with lower suicide rate after adjustment of potential confounding factors.
Method: From 2010 to 2013, 274 mean lithium levels of 434 lithium samples in drinking water were examined in relation to suicide standardized mortality ratios (SMRs) in 274 municipalities of Kyushu Island in Japan. Weighted least squares regression analysis adjusted for the size of each population was used to investigate the association of lithium levels with suicide SMRs. The associations of lithium levels in drinking water with suicide SMRs (total, male, and female) were investigated adjusting for proportion of elderly people, proportion of 1-person households, proportion of people with college education or more, and proportion of people engaging in primary industry (adjusted model 1), and further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature, and annual postal savings per person (adjusted model 2).
Results: Lithium levels in drinking water were significantly (β = −.169, P = .019) and inversely associated with male suicide SMRs but not total or female SMRs in the adjusted model 2.
Conclusions: The present findings suggest that lithium in drinking water may be associated with the low risk of male suicide in the general population. Further studies are required to confirm these findings and investigate gender differences.
J Clin Psychiatry 2015;76(3):319-326
© Copyright 2015 Physicians Postgraduate Press, Inc.
Submitted: April 24, 2014; accepted July 25, 2014.
Online ahead of print: February 3, 2015 (doi:10.4088/JCP.14m09218).
Corresponding author: Takeshi Terao, MD, PhD, Department of Neuropsychiatry, Oita University Faculty of Medicine 1-1 Idaigaoka, Hasama-machi, Yufu City, Oita Prefecture, 879-5593, Japan ([email protected]).
Suicide is an unresolved and serious problem in psychiatry. Several meta-analyses1-3 have shown antisuicidal effects of lithium in people with mood disorders, namely major depression and bipolar disorder, but these reviews have examined only randomized controlled trials that primarily compare lithium with placebo or other drugs in long-term prophylactic treatment of mood episodes (ie, not antisuicidal effects) that were maintained at so-called therapeutic levels. To date, there are only 2 studies4,5 that have directly compared antisuicidal effects (but not prophylactic effects). In one 1-year double-blind randomized controlled trial,4 patients with affective spectrum disorder and a recent suicide attempt were randomly assigned to lithium or placebo addition. Although survival analysis showed no significant difference of suicidal acts between lithium and placebo addition, post hoc analysis revealed that all completed suicides had occurred in placebo addition but not in lithium addition with significant difference. In another 2.5-year double-blind randomized controlled trial,5 patients with bipolar disorder and past suicide attempts were randomly assigned to treatment with lithium or valproate conditions, but no significant difference between the 2 treatments was found in either time to suicide attempt or number of suicide events.
In contrast, there is growing evidence from epidemiologic studies that lithium in drinking water may protect against suicide. An inverse association between lithium levels in drinking water and suicide rates was first reported in the United States in 27 Texas counties.6 In Japan, we showed the inverse association between lithium levels in drinking water and suicide rates for 18 municipalities of Oita prefecture,7 whereas another study8 found no association for 47 subdivisions in the East of England.8 A nationwide Austrian study,9 however, found an inverse association between lithium levels in drinking water and suicide rates after adjustment of population density, per capita income, and proportion of Roman Catholics, as well as the availability of mental health service providers. Recently, the Austrian group confirmed an inverse association between lithium levels in drinking water and suicide rates after adjustment of county-based population density, age, gender, race/ethnicity, median income per household, poverty, and unemployment rates in Texas.10 Very recently, 2 studies that were performed in Hirosaki prefecture of Japan11 and in 34 prefectures of Greece12 also confirmed the inverse association between lithium levels in drinking water and suicide rates.
To appropriately analyze such data, it is important to select potential factors to adjust the crude association between lithium levels in drinking water and suicide rates. With regard to the potential factors associated with suicide, it has been variously reported that greater suicidality was associated with male gender,13-15 female gender,15 older age,14 younger age,13,16,17 married status,15,18 unmarried status,15 outpatient service,19 unemployment,13,15,18,20,21 lower income,15,18 more sunshine,22 less sunshine,23 lower temperature,24 higher temperature,25 alcohol dependence,26 and lower omega-3 fatty-acids.27 As a preliminary study,28 apart from lithium in drinking water, we attempted to create a statistical model whereby suicide rate in 2008 was predicted by potential risk factors recorded from 1 year before (ie, 2007), which included the above personal and interpersonal factors, medical factors, economic factors, climate factors, alcoholic factors, and omega-3 fatty-acid factors in all the 47 prefectures in Japan. As a result, Japanese male suicide standardized mortality ratios (SMRs) in 2008 were accounted for by greater unemployment, higher proportion of elderly people, lower annual rate of marriage, and less annual postal savings per person in 2007, whereas female suicide SMRs in 2008 were accounted for by higher unemployment rate and lower annual mean temperature in 2007.28

- Lithium in drinking water may be associated with low risk of male suicide in the general population.
- Despite low lithium levels in drinking water, long-term intake of lithium via drinking water may be associated with the lithium effects on suicide in the general population.
- Antiaggressive effects rather than mood-stabilizing effects of lithium may be associated with the low risk of male suicide.
Therefore, it seems reasonable that these factors are selected as potential factors to adjust the crude association between lithium levels in drinking water and suicide rates in Japan. In addition, it is generally accepted that age, environment, educational background, and professions are associated with suicide. In the present study, the association of lithium levels in drinking water with suicide SMRs (total, male, and female) were investigated by adjusting for proportion of elderly people as one of age factors, proportion of 1-person households as one of environment factors, proportion of people with college education or more as one of educational background factors, and proportion of people engaging in primary industry such as farmer, fisherman, and forest workers as one of profession factors; further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature, and annual postal savings per person.
METHOD
Study Population
Japan has 4 large islands—Hokkaido, Honshu, Shikoku, and Kyushu. The northernmost island is Hokkaido, whereas the southernmost island is Kyushu. In the present study, we focused on Kyushu Island as the development of our previous study,7 which investigated Oita Prefecture, which was 1 of 8 prefectures in Kyushu Island. In 2011, the total, male, and female populations of Kyushu Island were 14,646,121, 6,952,255, and 7,693,866, respectively. Kyushu Island has 118 cities, 119 towns, and 37 villages, totaling 274 municipalities. Of the 274 municipalities, Fukuoka city had the largest population (1,409,297 residents), whereas Mishima village had the smallest population (366 residents). The difference of population was very large across the 274 municipalities. These data were acquired from the Ministry of Internal Affairs and Communications, Tokyo, Japan.
Suicide Data
Taking the large differences in gender and age distribution of individual municipality populations into account, the SMR of suicide in 2011 was calculated for each individual municipality. The standardized mortality ratio is an indirect method of adjusting a mortality rate, defined as the number of observed deaths in an individual municipality population divided by the number of expected deaths compared with the gender- and age-matched general population. We examined data from the Ministry of Health Labor and Welfare, Tokyo, Japan, on suicide and from the Statistics Bureau, Ministry of Internal Affairs and Communications, and then calculated total, male, and female suicide SMRs for 2011 across all the 274 municipalities.
Measurement of Lithium Levels in Drinking Water
From 2010 to 2013, 434 tap water samples (mainly, from the main rail station or the municipal office) of each municipality were taken and their lithium levels were measured by using mass spectroscopy analyzed by a third party. This method can measure very small amounts of lithium; the minimal amount of lithium that can be measured is 0.1 parts per billion (0.1 μg/L). If lithium levels in drinking water were measured at multiple points in the same municipality, the mean value was calculated. Although lithium levels were measured once, we confirmed a very small fluctuation in levels because the correlation coefficient between the lithium levels and those remeasured after 1 year in the same places was 0.998.7
Adjustment Factors
Although we initiated a crude model of the association of lithium levels in drinking water and suicide SMRs (total, male, and female) without any adjustment of the confounding factors (crude model), as aforementioned, the associations were further investigated by adjusting for proportion of elderly people, proportion of 1-person households, proportion of people with college education or more, and proportion of people engaging in primary industry (adjusted model 1). Finally, further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature, and annual postal savings per person (adjusted model 2).
Although the data of proportion of elderly people, proportion of 1-person households, proportion of people with college education or more, proportion of people engaging in primary industry, overall unemployment rate, and annual marriage rate in 2010 were available for all 274 municipalities from the Statistics Bureau, Ministry of Internal Affairs and Communications, the data relating to annual postal savings per person were only partially available in 2009 for 153 of 274 municipalities from the Statistics Bureau, Ministry of Internal Affairs and Communications, but not for the years 2010 or 2011. On the other hand, the data relating to annual mean temperature was partially available for 102 of 274 municipalities in 2010 from Japan Meteorological Agency, which was assumed to represent the neighboring municipalities and was extrapolated to the other municipalities where data were unavailable.
Statistical Analysis
When a procedure that treats all of the data equally would give less precisely measured data points more influence than they are entitled to and, vice versa, would give highly precise data points too little influence, weighted least squares regression analysis was performed by attempting to give each data point its proper influence over the parameter estimates. Also in the present study, due to greater differences in population size across the 274 municipalities, weighted least squares regression analysis adjusted for the size of each population was used to investigate the association of lithium levels in drinking water with the suicide SMRs.
Multiple regression analyses were used to predict suicide SMRs (total, male, and female) in 2011 by lithium levels in drinking water and the adjustment factors in 2010 and annual postal savings per person in 2009, which was similar to our previous method.28
This study was approved by the ethics committee of Oita University Faculty of Medicine, Oita, Japan.
RESULTS
Suicide Data
In 2011, 3,485 deaths in the total population (N = 14,646,121; 23.8 per 100,000 population), 2,456 deaths in the male population (n = 6,952,255; 35.3 per 100,000 population) and 1,029 deaths in the female population (n = 7,693,866; 13.4 per 100,000 population) were by suicide in Kyushu island.
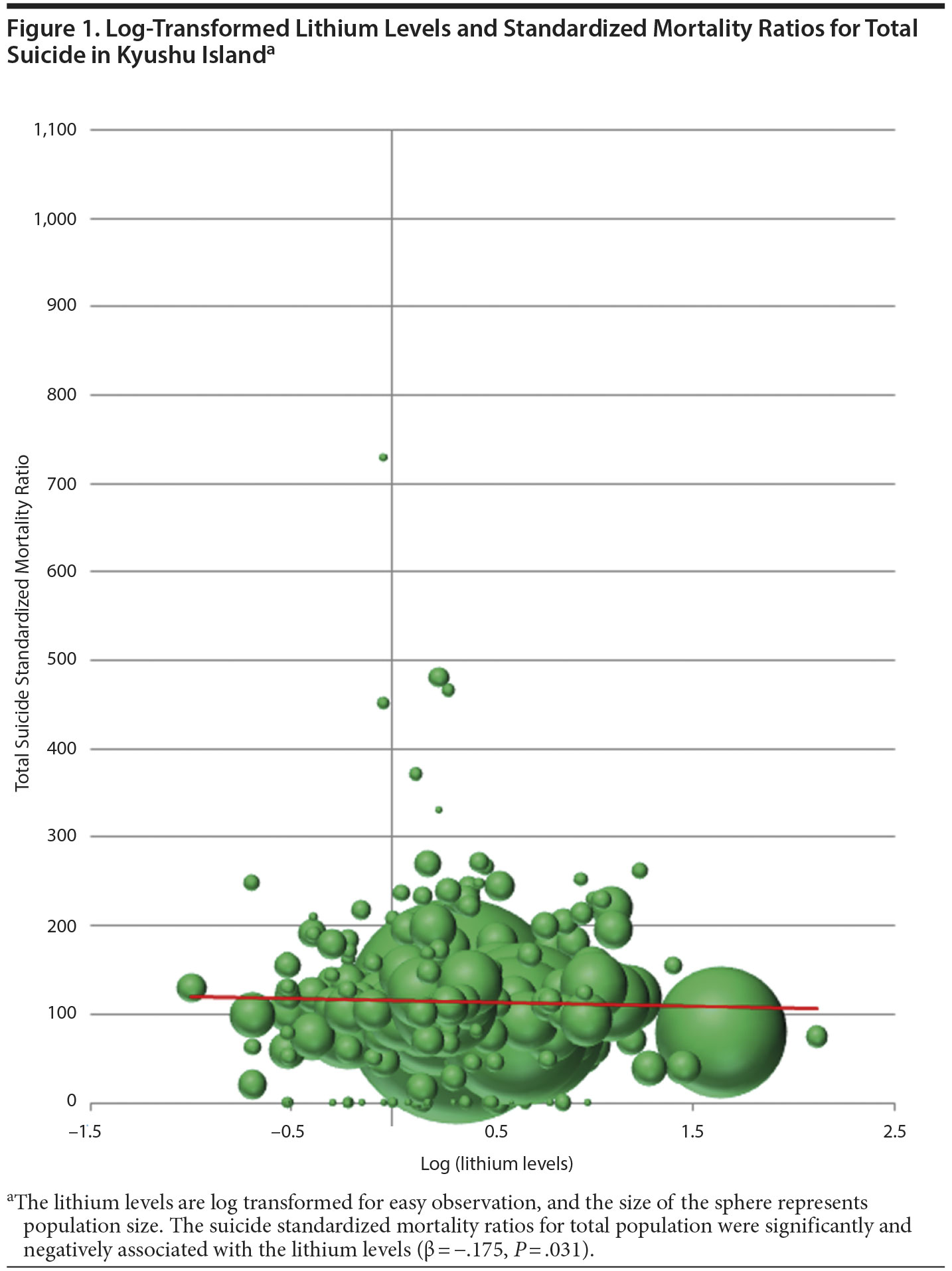
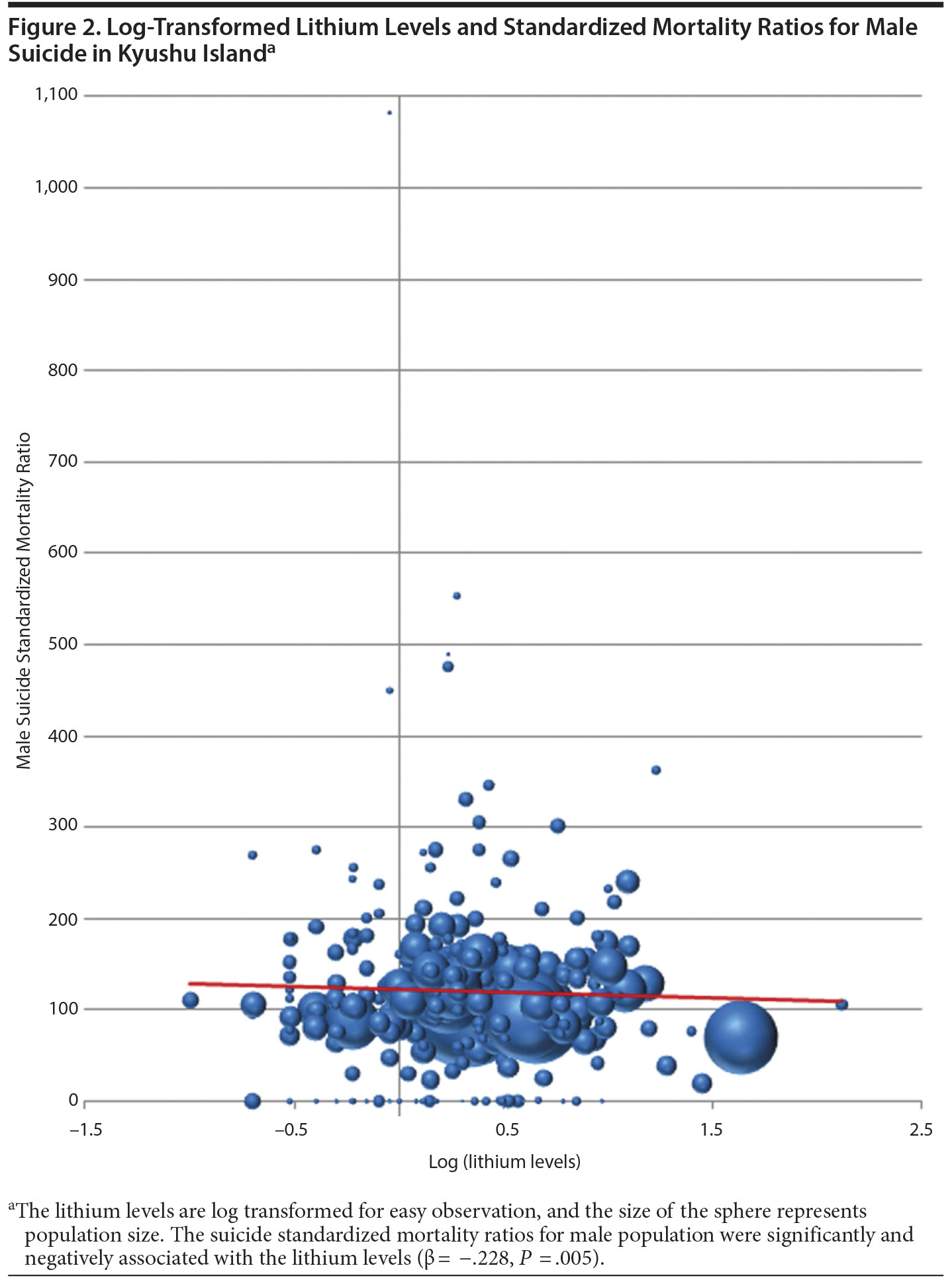
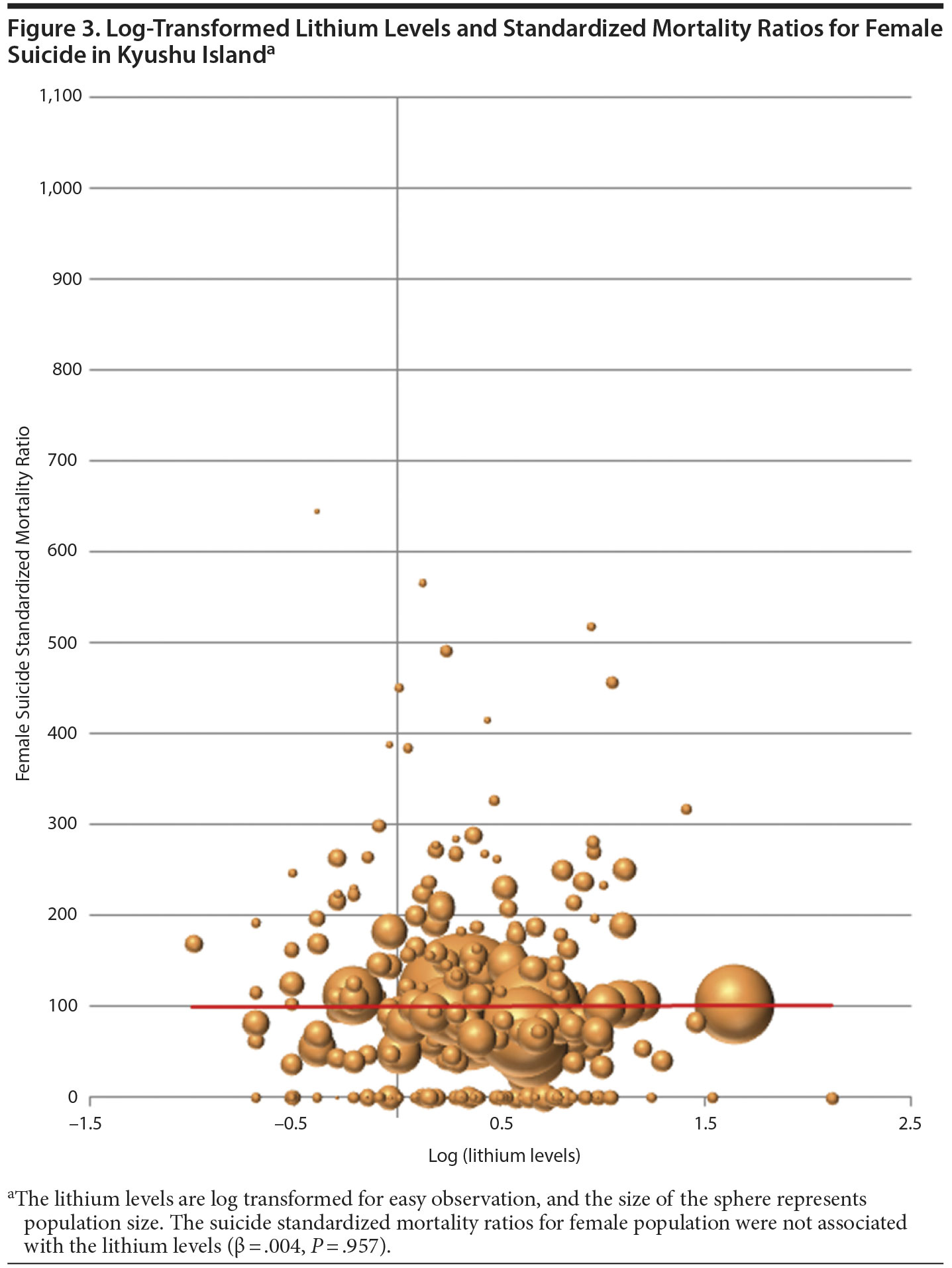
The mean total, male, and female suicide SMRs were 114 (SD = 84; range, 0-729), 120 (SD = 102; range, 0-1,082), and 101 (SD = 108; range, 0-644), respectively.
Lithium Levels in Drinking Water
The mean lithium level in drinking water of 274 municipalities of Kyushu Island was 4.2 μg/L (SD = 9.3; range, 0-130).
Adjustment Factors
The mean total, male, and female proportions of elderly people in 2010 were 27.7% (SD = 6.4; range, 14.0-43.4), 23.5% (SD = 5.3; range, 12.1-38.1), and 31.5% (SD = 7.4; range, 15.3-49.4). Mean proportions of 1-person households (per municipality households) in 2010, people with college education or more (per municipality population ≥ 15 years old) in 2010, and people engaging in primary industry (per municipality population ≥ 15 years old) in 2010 were 27.2% (SD = 7.6; range, 14.4-61.6), 19.1% (SD = 5.5; range, 7.1-36.9), and 6.8% (SD = 5.4; range, 0.2-23.6). The mean total, male, and female proportions of overall unemployment rate in 2010 was 7.5% (SD = 2.9; range, 0.8-20.3), 9.2% (SD 3.6; 0.6-24.4), and 5.1% (SD = 2.2; range, 0.8-15.0). Furthermore, the mean total annual marriage rate in 2010 was 4.8% (SD = 1.2; range, 1.4-9.6), annual mean temperature in 2010 was 17.7°C (SD = 2.7; range, 10.1-24.6), and annual mean postal savings per person in 2009 was Â¥2,261,700 (US $19,122) (SD = Â¥1,081,000 [US $9,139]; range, Â¥194,000-Â¥5,586,000 [US $1,640-$47,228]).
The Association Between Suicide SMRs and Lithium Levels
As shown in Figures 1, 2, and 3, total and male suicide SMRs, but not female SMRs, were significantly and inversely associated with lithium levels in drinking water in the crude model. As shown in Tables 1, 2, and 3, when the associations were further investigated adjusting for proportion of elderly people, proportion of 1-person households, proportion of people with college education or more, and proportion of people engaging in primary industry (adjusted model 1), total and male suicide SMRs, but not female suicide SMRs, were significantly and inversely associated with lithium levels in drinking water. After further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature and annual postal savings per person (adjusted model 2), male suicide SMRs, but not total or female suicide SMRs, were significantly and inversely associated with lithium levels in drinking water.
Click figure to enlarge
Click figure to enlarge
Click figure to enlarge

Click figure to enlarge

Click figure to enlarge

Click figure to enlarge
In the adjusted model 2, total suicide SMRs were significantly and directly associated with proportion of 1-person households, proportion of people engaging in primary industry, and overall unemployment rate. Also in the adjusted model 2, male suicide SMRs were significantly and directly associated with proportion of people engaging in primary industry and overall unemployment rate, while they were significantly and inversely associated with lithium levels in drinking water. In the adjusted model 2, however, female suicide SMRs were significantly and directly associated with proportion of 1-person households.
There was no multicollinearity in all multiple regression analyses.
DISCUSSION
In the present study, lithium levels were significantly and inversely associated with total suicide SMRs across 274 municipalities in Kyushu Island in the crude model, which is in agreement with our previous study.7 Moreover, male but not female suicide SMRs were significantly and inversely correlated with lithium levels in the adjusted model 1, where the associations were further investigated adjusting for proportion of elderly people, the proportion of 1-person households, proportion of people with college education or more, and proportion of people engaging in primary industry. However, in the adjusted model 2, where further adjustment was performed with overall unemployment rate, annual marriage rate, annual mean temperature, and annual postal savings per person, male suicide SMRs, but not total or female suicide SMRs, remained significantly and inversely associated with lithium levels in drinking water. These findings suggest that male suicide SMRs may be inversely associated with lithium levels in drinking water and that the combination of the significant association of lithium with male suicide SMRs and the nonsignificant association of lithium with female SMRs might have produced significant associations of lithium with total suicide SMRs in the crude model and the adjusted model 1 but not in the adjusted model 2.
To the best of our knowledge, this is the first report demonstrating a gender difference of the inverse association between suicide rate and lithium levels in drinking water. Although there has been a report showing little gender difference in clinical response to lithium treatment of bipolar and related affective disorders,29 with regard to suicide, among the lithium-unexposed population men had a 3.57-fold higher rate (95% CI, 3.12-4.07) of suicide than women, whereas, among patients purchasing lithium, the rate of suicide did not differ significantly for men and women.30 This report may indirectly indicate the gender difference in the antisuicidal effect of lithium treatment (ie, the antisuicidal effect for men is greater than that for women), which is in agreement of our study’s findings.
The present findings suggest that even very low lithium levels (mean = 4.2 μg/L) may be associated with a low risk of suicide and that within the lithium level range (0-130 μg/L) there seems to be a dose-response relationship with SMRs. In a routine psychiatric setting, we prescribe about 600-1,000 mg per day of lithium to our patients, producing approximately 0.4-1.0 mEq/L of therapeutic lithium levels for mood-stabilizing effects. If we were to prescribe 4.2 μg/L of drinking water to attain 600 mg/d of lithium, we calculate that the patient would need to drink 142,857 L of drinking water per day. A 4-week, randomized placebo-controlled study31 was conducted in which 400 μg of lithium or placebo was administered to former drugs users. Some subjects were violent offenders or had a history of domestic violence. Although serum lithium levels were not measured, the dose was 1/1,000 of clinically used doses. As a result, the mood test scores of the lithium group improved steadily and significantly, whereas those of the placebo group showed no consistent changes,31 revealing a possibility that very low doses of lithium can bring about mood-stabilizing effects. Nonetheless, it is likely that antiaggressive effects of lithium could potentially prevent suicide in those who take lithium contained in drinking water for a long time.32,33 If male aggression is greater and more responsive to lithium than female aggression, this could explain gender differences in the present findings, but more studies are required to further investigate this possibility.
In Texas, Dawson et al34 reported that the urine lithium was inversely correlated at statistically significant levels with all and first admission rates, with psychotic and neurotic rates, and with annual rainfall, and urine lithium level was positively correlated with water lithium level. Because the soils of several areas of Texas contained high levels of lithium salts and the rainfall washes the lithium from the soils and dilutes the surface water lithium levels, the relationship between rainfall and lithium levels in drinking water as well as mental admission may be thus explained.34 Such a mechanism can account for the difference of lithium levels in drinking water in Kyushu Island. In addition, it seems possible that hot spring may be associated with the soils containing high levels of lithium salts because Oita prefecture has several hot springs and high lithium levels in drinking water, and their relationship is yet to be determined.
The limitations of the present study are the lack of data relating to lithium levels in food and the proportion of the population who drank tap water and their consumption habits. Moreover, there is no evidence that water drinking habits were similar in these municipalities because, in some areas, residents might not drink tap water because of water quality. Moreover, it is unknown how many populations shifted within and out of municipalities and how long they drank tap water within their municipality. Finally, this type of study has a possibility of ecological fallacy inevitably, and we should understand the present results cautiously. To resolve these limitations, we are now performing a comparison study of serum lithium levels in suicide attempters and a control group.
CONCLUSIONS
The present findings suggest that lithium in drinking water may be associated with the low risk of male suicide in the general population. Further studies are required to confirm these findings and investigate gender differences.
Drug names: lithium (Lithobid and others).
Author affiliations: Department of Neuropsychiatry, Oita University, Oita City (Drs Ishii, Terao, Araki, Kohno, Shiotsuki, Hatano, Makino, and Kodama and Mr Mizokami); and Department of Clinical Psychology, Hiroshima International University, Hiroshima (Dr Iwata), Japan.
Author contributions: Drs Ishii and Terao performed literature search, study design, data collection, data analysis, data interpretation, and writing. Drs Araki, Kohno, Shiotsuki, Hatano, Makino, Kodama, and Iwata and Mr Mizokami contributed to data collection, data interpretation, and writing. Dr Ishii contributed to data analysis and writing. All authors contributed to and reviewed the final report.
Potential conflicts of interest: The authors report no financial or other relationships relevant to the subject of this article.
Funding/support: This work was supported in part by the Japanese Society for the Promotion of Science as Grant-in-Aid for Scientific Research (C) (22591264; Dr Ishii).
Role of the sponsors: The study sponsor had no role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Acknowledgments: The authors thank the municipalities for kindly sending drinking water for this study.
Additional information: The original data set for this study is available from http://www.soumu.go.jp/menu_news/s-news/01gyosei02_02000032.html for populations of municipalities, from http://www.e-stat.go.jp/SG1/estat/List.do?bid=000001048449&cycode=0 for elderly people, from http://www.e-stat.go.jp/SG1/estat/List.do?bid=000001048449&cycode=0 for 1-person households, from http://www.e-stat.go.jp/SG1/chiiki/Welcome.do?lang=01 and http://www.e-stat.go.jp/SG1/chiiki/ToukeiDataSelectDispatchAction.do for people with college education or more, from http://www.e-stat.go.jp/SG1/estat/List.do?bid=000001048449&cycode=0 for proportion of people engaging in primary industry, from http://www.e-stat.go.jp/SG1/estat/List.do?bid=000001048449&cycode=0 for overall unemployment rate, from http://www.e-stat.go.jp/SG1/estat/List.do?bid=000001048449&cycode=0 for annual marriage rate, from http://www.e-stat.go.jp/SG1/estat/NewList.do?tid=000001037021 for annual postal savings per person, and from http://www.jma.go.jp/jma/menu/report.html for annual mean temperature.
REFERENCES
1. Cipriani A, Pretty H, Hawton K, et al. Lithium in the prevention of suicidal behavior and all-cause mortality in patients with mood disorders: a systematic review of randomized trials. Am J Psychiatry. 2005;162(10):1805-1819. doi:10.1176/appi.ajp.162.10.1805 PubMed
2. Baldessarini RJ, Tondo L, Davis P, et al. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord. 2006;8(5, pt 2):625-639. doi:10.1111/j.1399-5618.2006.00344.x PubMed
3. Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346(4):f3646. doi:10.1136/bmj.f3646 PubMed
4. Lauterbach E, Felber W, Müller-Oerlinghausen B, et al. Adjunctive lithium treatment in the prevention of suicidal behaviour in depressive disorders: a randomised, placebo-controlled, 1-year trial. Acta Psychiatr Scand. 2008;118(6):469-479. doi:10.1111/j.1600-0447.2008.01266.x PubMed
5. Oquendo MA, Galfalvy HC, Currier D, et al. Treatment of suicide attempters with bipolar disorder: a randomized clinical trial comparing lithium and valproate in the prevention of suicidal behavior. Am J Psychiatry. 2011;168(10):1050-1056. doi:10.1176/appi.ajp.2011.11010163 PubMed
6. Schrauzer GN, Shrestha KP. Lithium in drinking water and the incidences of crimes, suicides, and arrests related to drug addictions. Biol Trace Elem Res. 1990;25(2):105-113. doi:10.1007/BF02990271 PubMed
7. Ohgami H, Terao T, Shiotsuki I, et al. Lithium levels in drinking water and risk of suicide. Br J Psychiatry. 2009;194(5):464-465, discussion 446. doi:10.1192/bjp.bp.108.055798 PubMed
8. Kabacs N, Memon A, Obinwa T, et al. Lithium in drinking water and suicide rates across the East of England. Br J Psychiatry. 2011;198(5):406-407. doi:10.1192/bjp.bp.110.088617 PubMed
9. Kapusta ND, Mossaheb N, Etzersdorfer E, et al. Lithium in drinking water and suicide mortality. Br J Psychiatry. 2011;198(5):346-350. doi:10.1192/bjp.bp.110.091041 PubMed
10. Blüml V, Regier MD, Hlavin G, et al. Lithium in the public water supply and suicide mortality in Texas. J Psychiatr Res. 2013;47(3):407-411. doi:10.1016/j.jpsychires.2012.12.002 PubMed
11. Sugawara N, Yasui-Furukori N, Ishii N, et al. Lithium in tap water and suicide mortality in Japan. Int J Environ Res Public Health. 2013;10(11):6044-6048. doi:10.3390/ijerph10116044 PubMed
12. Giotakos O, Nisianakis P, Tsouvelas G, et al. Lithium in the public water supply and suicide mortality in Greece. Biol Trace Elem Res. 2013;156(1-3):376-379. doi:10.1007/s12011-013-9815-4 PubMed
13. Hawton K, van Heeringen K. Suicide. Lancet. 2009;373(9672):1372-1381. doi:10.1016/S0140-6736(09)60372-X PubMed
14. Chen VCH, Tan HKL, Chen C-Y, et al. Mortality and suicide after self-harm: community cohort study in Taiwan. Br J Psychiatry. 2011;198(1):31-36. doi:10.1192/bjp.bp.110.080952 PubMed
15. Wei KC, Chua HC. Suicide in Asia. Int Rev Psychiatry. 2008;20(5):434-440. doi:10.1080/09540260802397446 PubMed
16. Hawton K, Saunders KEA, O’ Connor RC. Self-harm and suicide in adolescents. Lancet. 2012;379(9834):2373-2382. doi:10.1016/S0140-6736(12)60322-5 PubMed
17. Pitman A, Krysinska K, Osborn D, et al. Suicide in young men. Lancet. 2012;379(9834):2383-2392. doi:10.1016/S0140-6736(12)60731-4 PubMed
18. Qin P, Agerbo E, Mortensen PB. Suicide risk in relation to socioeconomic, demographic, psychiatric, and familial factors: a national register-based study of all suicides in Denmark, 1981-1997. Am J Psychiatry. 2003;160(4):765-772. doi:10.1176/appi.ajp.160.4.765 PubMed
19. Pirkola S, Sund R, Sailas E, et al. Community mental-health services and suicide rate in Finland: a nationwide small-area analysis. Lancet. 2009;373(9658):147-153. doi:10.1016/S0140-6736(08)61848-6 PubMed
20. Yur’ yev A, Vפrnik A, Vפrnik P, et al. Employment status influences suicide mortality in Europe. Int J Soc Psychiatry. 2012;58(1):62-68. PubMed
21. Motohashi Y. Suicide in Japan. Lancet. 2012;379(9823):1282-1283. doi:10.1016/S0140-6736(11)61130-6 PubMed
22. Vyssoki B, Praschak-Rieder N, Sonneck G, et al. Effects of sunshine on suicide rates. Compr Psychiatry. 2012;53(5):535-539. doi:10.1016/j.comppsych.2011.06.003 PubMed
23. Terao T, Soeda S, Yoshimura R, et al. Effect of latitude on suicide rates in Japan. Lancet. 2002;360(9348):1892. doi:10.1016/S0140-6736(02)11761-2 PubMed
24. Tsai J-F. Socioeconomic factors outweigh climate in the regional difference of suicide death rate in Taiwan. Psychiatry Res. 2010;179(2):212-216. doi:10.1016/j.psychres.2008.06.044 PubMed
25. Kim Y, Kim H, Kim D-S. Association between daily environmental temperature and suicide mortality in Korea (2001-2005). Psychiatry Res. 2011;186(2-3):390-396. doi:10.1016/j.psychres.2010.08.006 PubMed
26. Manoranjitham SD, Rajkumar AP, Thangadurai P, et al. Risk factors for suicide in rural south India. Br J Psychiatry. 2010;196(1):26-30. doi:10.1192/bjp.bp.108.063347 PubMed
27. Lewis MD, Hibbeln JR, Johnson JE, et al. Suicide deaths of active-duty US military and omega-3 fatty-acid status: a case-control comparison. J Clin Psychiatry. 2011;72(12):1585-1590. doi:10.4088/JCP.11m06879 PubMed
28. Ishii N, Terao T, Araki Y, et al. Risk factors for suicide in Japan: a model of predicting suicide in 2008 by risk factors of 2007. J Affect Disord. 2013;147(1-3):352-354. doi:10.1016/j.jad.2012.11.038 PubMed
29. Viguera AC, Tondo L, Baldessarini RJ. Sex differences in response to lithium treatment. Am J Psychiatry. 2000;157(9):1509-1511. doi:10.1176/appi.ajp.157.9.1509 PubMed
30. Kessing LV, S׸ndergץrd L, Kvist K, et al. Suicide risk in patients treated with lithium. Arch Gen Psychiatry. 2005;62(8):860-866. doi:10.1001/archpsyc.62.8.860 PubMed
31. Schrauzer GN, de Vroey E. Effects of nutritional lithium supplementation on mood: a placebo-controlled study with former drug users. Biol Trace Elem Res. 1994;40(1):89-101. doi:10.1007/BF02916824 PubMed
32. Terao T, Goto S, Inagaki M, et al. Even very low but sustained lithium intake can prevent suicide in the general population? Med Hypotheses. 2009;73(5):811-812. doi:10.1016/j.mehy.2009.02.043 PubMed
33. Terao T. Aggression, suicide, and lithium treatment. Am J Psychiatry. 2008;165(10):1356-1357, author reply 1357. doi:10.1176/appi.ajp.2008.08040598 PubMed
34. Dawson EB, Moore TD, McGanity WJ. Relationship of lithium metabolism to mental hospital admission and homicide. Dis Nerv Syst. 1972;33(8):546-556.PubMed
Please sign in or purchase this PDF for $40.00.
![]() Save
Save
![]() Share
Share
![]() Cite
Cite
